SIBO, or Small Intestinal Bacterial Overgrowth, is a digestive disorder where too many bacteria, especially the wrong types, grow in the small intestine, leading to symptoms like bloating, gas, diarrhea, abdominal pain, fatigue, and nutrient malabsorption.
Normally, the small intestine is much lower in bacteria than the large intestine. SIBO occurs when there are noticeably more bacteria there than normal.
In certain areas of the wellness community, SIBO is frequently presented as the root cause of a lot of digestive issues. Meanwhile, the evidenced based medical community tends to be a bit more cautious with diagnosing it.
This post will explore a bit of a balanced take on this topic, as well as summarise how to treat it.
Symptoms
Symptoms of SIBO vary depending on the severity of the overgrowth and the type of gases being produced. They are often categorized into digestive symptoms and systemic effects caused by malabsorption.
Common Digestive Symptoms
- Abdominal bloating
- Excessive gas and flatulence. This is caused by bacteria fermenting carbohydrates in the small bowel.
- Abdominal pain and cramping
- Alterations in bowel habits. This could be either diarrhea or constipation.
- Nausea
- Sensation of excessive fullness: Even after eating small or moderate-sized meals.
Signs of Malabsorption (More Severe Cases)
- Steatorrhea: Fatty, oily, or floating stools caused by the breakdown of bile salts by bacteria.
- Unintended weight loss: Due to the inability to properly absorb macronutrients.
- Fatigue and “brain fog”: Often linked to the metabolic byproducts of the bacteria or nutrient deficiencies.
- Nutrient deficiencies: Including iron and vitamins B12, A, D, E and K.
What Causes SIBO
SIBO is generally somewhat of a secondary condition. It’s something that occurs when symptom that one or more of your body’s natural protective mechanisms have failed. To effectively treat SIBO, you often have to identify which of these “gut defences” has broken down.
Common causes include:
- Impaired Motility: If the rate of food moving through the small intestine slows down too much, bacteria have time to anchor and multiply.
- Post-infectious IBS: Nerve damage following a bout of food poisoning can reduce motility.
- Gastroparesis: Slowed stomach emptying, often linked to diabetes or viral infections.
- Hypothyroidism: Low thyroid function can slow down the entire digestive tract.
- Abdominal Surgery: Scar tissue from past surgeries or procedures like gastric bypass can create “blind loops” where food and bacteria get trapped.
- Strictures: Narrowing of the bowel, often seen in Crohn’s disease.
- Diverticula: Small pouches in the small intestine wall that provide a breeding ground for bacteria.
- Ileocecal Valve Dysfunction. If the valve between the small and large intestine doesn’t close properly, colonic bacteria can “backflow” into the small bowel.
- Low Stomach Acid: Stomach acid kills most bacteria before they reach the small intestine. Long-term use of Proton Pump Inhibitors (PPIs) or conditions like H. pylori can lower this defence.
- Bile Acid or Enzyme Deficiencies: Bile and pancreatic enzymes have antimicrobial properties. Conditions like chronic pancreatitis or gallbladder issues can reduce their effectiveness.
- Diabetes: High blood sugar can cause autonomic neuropathy, damaging the nerves that control gut transit.
- Celiac Disease: Chronic inflammation and damage to the small intestinal lining can reduce motility.
- Scleroderma: A connective tissue disorder that can lead to significant motility issues throughout the GI tract.
How is SIBO Diagnosed
One of the biggest barriers in this area is that there is not a gold standard diagnostic criteria for SIBO.
There are two main ways of testing for SIBO, and they are often combined with other assessments.
Test One: Breath Testing

This test involves and measuring the amount hydrogen or methane that you breathe out after drinking a mixture of glucose or lactulose and water. If they rise rapidly, it can indicate bacterial overgrowth in the small intestine.
Test Two: Small Intestine Aspirate

This is test directly measures the presence of bacteria rather than their gas byproducts. It is far more invasive though.
It usually involves an endoscopy. While the patient is sedated, a gastroenterologist passes a thin, flexible tube through the mouth and stomach into the small intestine. A small amount of fluid is suctioned out, which is then sent to a microbiology lab to see how many bacterial colonies grow.
Flaws in Both Tests
Neither of the primary testing methods is perfect. Here is why evidence-based clinicians often view these with some level of scepticism.
The Flaws in Breath Testing
- There is a high false positive rate. If you have “fast transit” (food moves quickly through your system), the test sugar may reach your colon too early. The bacteria in your colon will ferment it, causing a gas spike that looks like SIBO but is actually just a normal, healthy colon.
- There is still no global agreement on the exact cutoff for a positive result, leading to different interpretations depending on which lab you use.
- Preparation Errors: The test is highly sensitive to what you ate the day before, whether you’ve exercised, or even if you’ve brushed your teeth right before the test.
- If using a Glucose test, the sugar is often absorbed before it reaches the end of the small intestine, meaning it may miss overgrowth located further down the tract.
The Flaws in Aspirate Testing:
- There is often contamination. It is nearly impossible to pass a tube through the mouth and throat without picking up “hitchhiker” bacteria, which can lead to a false positive.
- SIBO isn’t always spread evenly. If the doctor suctions fluid from a “clean” spot but the overgrowth is slightly further down, the test will be a false negative.
- Many gut bacteria die when exposed to oxygen. If not handled in a perfectly oxygen-free environment, the bacteria may die before they can be counted.
- Because it requires an endoscopy and sedation, the risk-to-reward ratio is often too high for a condition that can usually be managed with less invasive measures.
Other Tools Used in Diagnosing SIBO
Since both of the above have flaws, often gastroenterologists will look at other variables as well which increase the odds. For example:
- Blood testing to look for vitamin deficiency
- Stool evaluation to test for fat malabsorption.
- Imaging tests, such as X-rays, CT scanning or MRI to look for structural abnormalities of the intestine.
Prevalence
Since there is no gold standard diagnostic criteria, the evidence on prevalence is fairly broad.
A meta-analysis found the following and other similar reviews have found estimates such as the below:
- Healthy Controls: 2.5% – 15%Age (Higher in 60+)
- IBS-D Patients: ~36%
- Diabetes: (Type 1 & 2) ~29%
- Celiac Disease: ~20%
- IBD (Crohn’s/UC): ~22% – 31% partly due to strictures and prior surgeries
A key note though is that 30% of healthy controls in that specific review also tested positive when using the Lactulose Breath Test. So you can see how relying on a breath test in isolation would lead to a lot of false positives.
Management
There are many ways to manage SIBO. And often it involves a combination of both medical approaches and nutrition.
Antibiotics

Antibiotics are typically the front-line approach to managing SIBO. This can directly reduce the overgrowth.
Options such as Rifamixin and Neomycin have quite high success rates (>60%) for normalising breath test results.
One big issue though is that ~45% of people have a recurrence of SIBO within 9 months of antibiotic use. And there are many downsides of doing repeated cycles of antibiotics.
So in a perfect world, identifying and addressing the root cause is important.
Root Cause Medical Management
The two main causes of SIBO tend to be related to slow motility, or low stomach acid. So if either of those are identified, they can often be addressed.
For example, sometimes people get surgery if it is a structural defect. Or prokinetics medication for speeding up motility. Or the removal of proton pump inhibitors or other medications that can reduce stomach acid.
There are many ways this can be done and there are options beyond what has been mentioned above. But it comes down to finding why SIBO occurred in the first place.
Nutritional Management
The main proposed methods for managing SIBO involve:
- Starving the bacteria of food it would normally eat
- Adding probiotics to get a better balance of good vs bad bacteria.
- Taking steps to manage the symptoms, such as the low FODMAP diet.
The Low FODMAP Diet
The low FODMAP diet is a short term dietary approach (with reintroduction phases) that reduces the amount of fermentable carbohydrates.
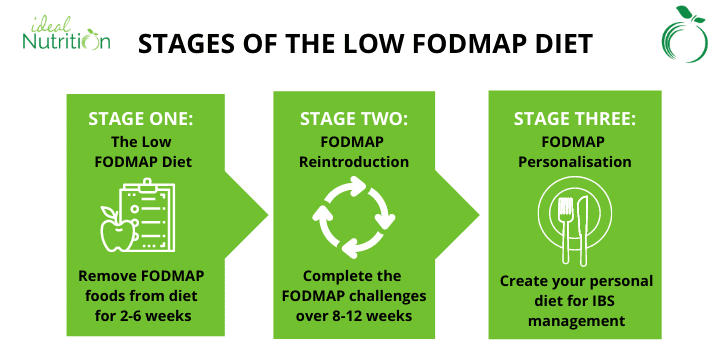
This directly can improve symptoms such as bloating and diarrhea. So, it can help manage symptoms of SIBO while it is present. Although the evidence is not super strong specifically for SIBO, since more research is on IBS in general.
Indirectly it has potential to reduce the bacterial overgrowth too by reducing the amount of fuel those bacteria has available.
This diet is not an appropriate strategy in isolation though since it likely will not reduce the overgrowth enough by itself.
The Elemental Diet
This is a more extreme nutritional intervention that is considered more effective, albeit it is also a short-term strategy.
It involves all solid food with a pre-digested liquid formula for 14–21 days. Because these nutrients (amino acids, simple sugars, fats) are absorbed within the first few centimetres of the small intestine, the bacteria further down have nothing to eat and essentially starve.
One study found a >80% success rate over that duration for normalising breath tests. Technically that’s even more effective than antibiotics.
That said it is not a commonly used protocol due to things such as cost, access, restriction and palatability.
Probiotics
This is the most controversial area of SIBO nutrition. Some argue that adding more bacteria to an overgrowth is “just adding MORE bacteria to an overgrowth” but the research is more nuanced.
Recent reviews suggest that certain strains such as Saccharomyces boulardii and Bacillus clausii can actually help clear SIBO and improve the effectiveness of antibiotics.
That said, some people find that multi-strain probiotics can worsen bloating and gas during the active overgrowth phase.
Timing can often matter. In practice we often use probiotics after a round of antibiotics to help restore balance and potentially help prevent recurrence.
What’s Evidence Based and What’s Not
It is clear that SIBO exists. That is not debateable.
What is not evidence based is simply diagnosing people based on a breath test, given the high false positive rates. That can lead to unnecessary treatment protocols; some of which can cause harm.
Using a mix of testing and assessing background gives a much higher likelihood of an accurate diagnosis.
If you suspect SIBO is at the heart of your digestive issues, the most effective path forward involves a three-pillar approach:
Pillar 1: Strategic Identification: Instead of just a breath test, ideally the clinician who interprets those results alongside your medical history, nutrient levels (like B12 and Iron), and potential risk factors.
Pillar 2: Use proven tools to reduce the bacterial load. While antibiotics like Rifaximin are the front-line clinical choice, dietary approaches such as the Elemental Diet remain effective nutritional alternatives.
Pillar 3: Addressing the “Why”: This is the most overlooked step. If you don’t identify why the bacteria migrated there in the first place, you face a 43.7% chance of recurrence within 9 months. Whether it’s managing motility with prokinetics or addressing a structural issue, fixing this is the only way to stay clear long-term.